We here today are the
winners in Life’s lottery – survivors of countless generations that preceded us
in the long arc of life embodiment. The ancestors of all life forms existent
now had to have themselves been the recipients of selective gifts sufficient to
grow to maturity and reproduce, thereby contributing their link in the chain of
continuum leading to today’s edition, here and now. In each generational step –
and long before human biomedicine advances – Mother Nature, through her wondrous
processes, selected those traits that would enhance the probability of survival
of each of her children, and supplied each with a set of adaptive survival
aids. All species existent today possess built-in efficient life management
strategies functioning wisely and automatically, safely hidden beyond conscious
control.
What follows, then, are
the interim results of our ongoing examination of this wondrous bequest,
referenced by the attributed findings of leading thinkers across many disciplines,
with leads to further material for more in-depth study by those interested in…
NATURE’S LIFE MANAGEMENT SYSTEM
(What the placebo response tells us)
[A placebo is a simulated or otherwise medically
ineffectual treatment for a disease or other medical condition, intended to trick the subject’s system with information so that it
believes the situation warrants a reduction in pain or the mounting of a
resource-expensive immune response. Often patients given a placebo
treatment will have a perceived or actual improvement in a medical condition, a
phenomenon commonly called the placebo response.]
I said
that the cure itself is a certain leaf, but in addition to the drug there is a
certain charm, which if someone chants when he makes use of it, the medicine
altogether restores him to health, but without the charm there is no profit
from the leaf. (Plato - Charmides).
Our remedies oft in ourselves do lie.
(William Shakespeare - All's Well That Ends Well)
Will science take the mystery out of healing? I don’t
believe so. I think there’s going to be an element of the shaman residing at
the core. My effort to do research in placebo is to acknowledge that core, not
to destroy it, because I don’t think it can be destroyed.
(Ted
Kaptchuk - Co-Director, Program in Placebo Studies, Harvard)
INDEX
THE ALLOPATHIC AND ALTERNATIVE MODELS
THE PLACEBO RESPONSE: EVOKING THE INTERNAL
HEALER
REPORTS FROM TO-DAYS EXPLORERS OF
LIFE’S INTERNAL HEALING MECHANISMS
SETTING THE STAGE:
Our interests in the
mysteries of healing processes deepened in January 1993 by a visit to observe
the curanderos plying their trade in San Juan Chamula, in the Chiapis
Highlands of Mexico, and then in Chichicastenango, Guatemala. The account of
our findings at that time is HERE, and it
attests to the power of belief and intention. Both of us had had secular upbringing
and were blessed with good health, only occasionally having had to resort to
western allopathic biomedical practitioners. We had earlier seen certain Hopi
and Navaho rituals in Arizona, and had often wondered between our selves as to
how our forebears had managed to cope without 19th and 20th
century advances in medical technology, but to actually see with our own eyes
people being ‘treated’ for their afflictions through the apparent agency of
faith, belief and ritual was mind opening. Over the next two years we read up
on shamanic processes and also became aware of many alternative healing
practices and belief systems, almost to the point of bewilderment in that it
seemed virtually anything had been or was currently employed somewhere
in the interest of curing and healing: visualization, chanting, dowsing,
aromatherapy, acupuncture, herbs, reflexology, iridology, fragrances, massage,
yoga, electromagnetic frequency generators, psychotherapy, prayer, Christian
Science, hypnosis, meditation, astrology, therapeutic touch and more.
The issue of health
attracts a lot of interest, and thus it is that there are many means toward the
same ends as that promised by traditional allopathic biomedicine, namely the
triggering of an afflicted person’s internal curing-healing mechanisms. In 1995
we traveled extensively, and amongst our experiences was a visit to Boston
‘Mother Church’ of Christian Science (where we had privileged discussions with
adherents from as far away as Australia),followed by a week in Salt Lake City
interacting with the LDS Mormons. That year we also spent two months combing
the archives of the Association for Research and Enlightenment (A.R.E.) in
Virginia Beach. (1)
What follows, then, are
the findings and reflections of two questers who are deeply in love with each
other, and with life; and just as any lover wants to know more of the beloved,
we are deeply curious about the vital forces of Nature, and attentive to the messages we pick up from the natural world. We live in a part of the
world that experiences the four-season effect – where nature cycles its
creatures through the perennial birth-maturation-contraction-dormancy
progression – the seed preserved to flower again at the sun’s bidding. It is
hard to imagine that all came about as a result of chance – the natural world
itself whispers of an implicit intelligence guiding the evolution of explicit manifestations of
itself, adapting to greater complexities and richer diversities. Just as we
look to our past to better understand our now, we naturally
project the arc into the future, and wonder… Yet the wonder also
embraces our realization that – within the beauties of beloved life – there are
harsh rigors involved in the birthing and recycling processes – and those
rigors attend the existence of the transient sun,
stars and galaxies, as well as continuance of all sentient life. Not being
certain as to the meaning of the Mystery, we can grant ourselves permission to
explore all possibilities, and wonder…
It was early January 1998, and they’d been back in Mexico for a
couple months, currently camping in their Coleman pop-up in a primitive sandbar
campground adjacent the fishing village of La Manzanilla, parked in a coconut
grove directly adjacent the Pacific Ocean. They’d been here on previous trips,
and as a result knew many of the other snowbird campers and local residents and
shopkeepers … some of their experiences in this delightful place are to be
found HERE , HERE and HERE.
Each dawn commenced with a 10km walking circuit, the return leg
of which was especially anticipated since it was along the beach back to the
camp and breakfast, and along the beach there might be an opportunity to
observe schools of sea bass cruising across the face of large incoming waves,
or sometimes a whale breaching further out in Bahia Tenacatita. One morning
before moving onto the beach he stepped into a grove of mesquite to have
a pee, and there was quite shaken to observe that his stream was coloured a
high crimson. His immediate thought was that it might be cancer, his mind
linking the symptom to a life-threatening incidence inflicted upon their eldest
son the prior year. It seemed that his energy emptied out of him along with the
fluid, and he was quite introspective during the remainder of that morning’s
walk. Later in the day, a sample of urine was shown to the lady doctor in the
fishing village, and she recommended an immediate consultation with specialists
at a private clinic-hospital in the city of Manzanillo, some 60 km south.
That afternoon they presented at the clinic, and perhaps because
of their touristo appearance (and hence probably representing an
insurable opportunity) they were quickly moved past the dozen or so Mexicanos
already queued in the reception room and – while a urine sample was being
analyzed by the clinic technicians – a very eager urology specialist who
fortunately was fluent in English conducted an interview. The urologist then
gravely perused the lab report, and he indicated that – in his professional
view – there was blood in the hombre’s urine. Seeing that we were all in
agreement thus far, he prescribed a strong laxative to be taken that day so as
to clean out the afflicted body overnight, followed by fasting until a
scheduled return visit the next morning when the urologist would administer an
IVP (intravenous pyelogram). This procedure comprised a dye inserted into a
vein, followed by the taking of an hour-long time-lapse series of X-rays to
image the urinary tract as it processed the dye and also to reveal any
obstructions in the system. Following the IVP procedure, the urologist
explained through graphics and the X-rays, what had occurred… the prostate
gland at the base of the bladder had became very enlarged over time, creating a
convexity in the bladder floor that had kept urine from being expelled, and in that
residue of urine, a quantity of stones had formed. A large quantity – 40 or so
showing on the X-rays – and apparently one of the stones had rattled against
another and split, with a piece then being small enough to enter and cut the
exit urethra on its passage the previous morning in the mesquite patch.
The Mexican urologist indicated that standard treatment called
for a downsizing of the prostate via TURP
– trans-urethral-resection of the prostate (essentially a roto-rooting
hollowing of the gland), and then a manual crushing of the stones and flushing
of the fragments – the whole procedure performed by going up through the
waterworks from outside. The urologist also noted that recovery rooms were
available at the hospital, since there would be post-procedural incapacitation
for a few days. He also advised that the patient’s insurance would take care of
the expenses, and that the procedure should be undertaken ASAP as otherwise
recurrence of the symptom could lead to infection. Perhaps it was weakness from
loss of blood, or from the purgative-fasting regime, or wariness from having
observed the peeling paint on the ceiling whilst undergoing the X-rays, or
simply being a Canuck chicken … but the thought arose that there must
be a better way, and our hero suddenly recalled (falsely) that his retirement
medical insurance was only valid domestically rather than abroad, so he would
have to take a rain-check to ponder the options. The urologist was obviously
disappointed, but on the settling of his account for services rendered over the
two visits, he agreed to release the X-rays for further study and possible
early reconsideration and return, or otherwise for assessment by doctors back
home.
It was another three months before the couple returned home,
after a second two month stopover in Virginia Beach to comb the A.R.E. archives
for leads on an earlier interest in electromagnetic (E-M) fields and energy
medicine, and along the way a few stones had been passed and retrieved. Another
month passed while being processed through the family doctor-urologist system,
another month in lab tests on the stones to determine composition, and a couple
months in delaying discussions with the urologist (Dan - not his real name). It
was recalled that both of the patient’s older brothers had underwent the TURP
procedure with serious, enduring post-op complications such as urinary
incontinence, sterility and impotence, complications that – Dan admitted – were
highly probable … but the stones had to come out, and they’d quickly re-form in
the bladder unless the prostate was downsized. In the meantime, Dan arranged
ultrasound imaging to calibrate the prostatic volume, and he also personally
examined the prostate-bladder via cystoscope, at the conclusion of which he
exclaimed to the attending nurse that “this bladder’s so full of stones it
looks like a bubble-gum machine”.
Ever since the January incident, the couple had been personally
researching alternative options, including discussions with homeopathic,
acupuncture, herbalist and naturopathic practitioners. They’d also continued
their main research of recent years, tracking down literature and contacts
pertaining to the electromagnetic work of Robert O. Becker, the extensive research by Professor Michael Persinger concerning magnetism and the brain,
the biofeedback-GSR studies of Elmer and Alyce Green and – following on a lead at A.R.E.,
they tried to locate a Danish-born, Toronto based electrical engineer and
inventor of numerous devices including a cigarette-pack sized 8 hertz pulsed
magnetic-field generator that ran on a nine volt battery and was used to
stabilized brain waves at the alpha state, inducing emotional and physical
well-being. This inventor was eventually tracked to his retirement home in a
community approx 100 kms away, and when he was telephoned and our interests
explained, he indicated that his inventions and related literature could be
accessed at his wife’s clinic in their nearby market town. We contacted his
wife Alice (not her real name) and drove over to view the products.
Our initial interest was deflected when we noticed that a rear
wall of Alice’s large office was taken up by a bank of five wooden cabinets on
which lights were blinking and several dials affixed, and from which a soft hum
emanated. In response to our queries, Alice indicated that these were radionic machines, and the devices were calibrated
so as to remotely treat her clients, some of whom were relatives as far distant
as Germany and Australia. The technology had been invented in the early 1900s
by a California alternative health practitioner n/o Albert Abrams who claimed
that a person normally maintains organic health through the brain’s employment
of discrete signals to each organ – each of which operates within its own
unique frequency range; for example all human livers respond to a ‘liver’
frequency, adjusted slightly because each body itself is unique. Disease or
dysfunction occurred when the brain’s guiding ‘signal line’ to its organs is
lost. Seeing that all parts of a body contain a record of the whole, diagnosis
and remedial treatment could be effected through a representative ‘witness’
from the host body, such as a hair clipping, blood sample, or nail clipping
which was placed in a ‘witness-well’ of the device. All but one of the device’s
dials would be set to the prescribed ‘frequency rates’ determined by Abrams
from tests on healthy subjects. The setting for the final dial was determined
through a focused dowsing operation by the operator who visualized the known
patient and – in stroking a rubberized ‘stick-pad’ whilst simultaneously
rotating the final dial – tuned in on the unique DNA frequency of the subject,
as represented by the ‘witness’… and started incrementally nudging the
dysfunctional organ to its generic rate.
[Some understand the rates as access codes to groups of
energy information patterns, themselves complex frequencies resonant with the
subtle energy fields of specific tissues, organs or pathologies – and that the
‘radionic’ phenomenon itself is a means of information transfer that informs
the patient’s system as to what it needs to bring itself into harmony. Others
believe the essence of radionics comprises the unity of operator and subject,
established by intent and facilitated by an instrument, and that the
fundamental activity behind the application of radionics is the operator’s
handling of consciousness.]
Alice was advised about the ongoing EM studies and the ARE
research, it also being mentioned that we’d came across references to Abrams
and radionics, but had thought that the process had been abandoned, and we’d
never expected to encounter an actual practitioner. Alice observed that she
herself had been an R.N. many years ago, but she’d developed cancer that
oncologists had diagnosed as terminal; she’d refused surgery/ radiation/ chemo
etc and healed herself through adjustment of life-style, visualizations and
treatments by a radionics practitioner. She had somehow managed to acquire an
‘Abrams box’ and her husband had replicated the device for use in her own
clinic, and he’d also made devices for the use of her students in their own
clinics in other communities.
She provided a list of authors dealing with the field, and we
subsequently accessed many of these books for our research. On the spur of the
moment, Alice was asked if she’d ever treated any patients for bladder stones
or enlarged prostate, and she was shown the Mexican X-rays and local ultrasound
and lab reports which for some reason had been dragged along; she answered in
the affirmative as to prostate, but in the negative as to stones - then checked
her Abrams rate book and said there was a rate indicated for stone elimination.
She said that – should radionic treatments ever be requested - the first couple
should be handled here in her office, with the patient sitting across the room
reading or whatever, where she could watch for any untoward reactions during
treatment; also the client should be accompanied by another person to drive him
home, as sometimes deep fatigue would be experienced afterwards. Later
treatments could be conducted remotely on demand, with the caveat about
subsequent weakness and fatigue as the client’s body readjusted.
A few weeks later and after research, Alice was contacted, a
hair sample given, and for the next hour her treatment procedures were observed
from across the room, with no wiring connected to the body. Alice applied
herself silently in very purposeful concentration and her confident,
professional approach bespoke of belief and intention in the same manner as
that earlier seen in the curanderos of Central America. Marnie was quite
interested in the process, and Alice showed her how the stick-pad worked. No
effects were felt during the treatment, but on the way home he was glad to not
be driving, and mainly slept then … and for the rest of that day.
Four days later (Oct 18th) Dan telephoned and said
that – after reviewing the file – he felt that he should perform a biopsy of
the prostate on the 20th, to ensure there was no malignancy. This
would be undertaken on an outpatient basis under full anesthetic, and since it
appeared to be a reasonable precaution, the procedure was booked. After the
biopsy, a second visit to Alice’s clinic occurred on Oct 30th, and
she was apprehensive concerning the biopsy, as colour had by then reappeared in
the urine. After treatment, he again slept on the way home, and the next day
was totally exhausted, with bladder spasms later commencing and attempts to
urinate every 15 minutes.
Over the next two days the spasms intensified and then
disorientation set in; by evening of the 4th day of blockage we went
to ER for catheterization. The ER staff was unable to insert a catheter, and
Dan was called in and finally he was able to force in a catheter; he expressed
his exasperation at the foot dragging to proceed with the TURP, and he was told
that the reason stemmed from concerns over the procedural side-effects; that
the physical expression of our love for each other was a most important aspect
of our lives; and that – even with the cramps etc. – last night we had made
love for possibly the last time and later wept together. Dan’s professionally
detached composure crumbled with empathy, and he said that he should
immediately schedule the TURP, but that he would modify the procedure to leave
sufficient prostatic tissue at the upper end to retain normal bladder sphincter
function.
About a week
later Dan performed the modified TURP. An epidural anesthetic allowed actual
observation of the resection and subsequent pulverization of the stones –
one-by-one – via laser lithotripsy. Afterwards, Dan came by the recovery room,
and – after providing assurances that everything had went as agreed – he
admitted to being very perplexed, saying “notwithstanding the X-ray
images and my own earlier scoping to fully evaluate the situation, plus
ultrasound imaging to measure prostate size, my findings during the actual
procedure were (i) the prostate was only half the expected size, and (ii) there
were only half as many stones present, and they were much smaller than
expected. So… do you have any idea as to what has happened??”
To which
there was no response, yet one could wonder…
THE ALLOPATHIC AND ALTERNATIVE MODELS
The western allopathic bio-medical infrastructure
in place today was mainly designed with infectious agents in mind. Physician
training and practices, hospitals, the pharmaceutical industry and health
insurance all were built around the model of running tests on sick patients to
determine which drug or surgical procedure would best deal with some discrete
offending agent. The model worked well for its original purpose, but medicine’s
triumph over infectious disease brought to the fore the so-called chronic,
complex diseases – heart disease, cancer, diabetes, Alzheimer’s and other
illnesses without a clear causal agent eg. 365 categories of pharmaceutically
treatable dysfunctions described in the evolving editions of The Diagnostic and
Statistical Manual of Mental Disorders. Now that we live longer, these typically
late-developing diseases have become our biggest health problems, and account
for three-quarters of health-care spending.
The
medical community knows that preventive action is the way to go – and aside
from getting people to stop smoking – the three most effective ways of lowering
the risk that these diseases will take hold in the first place, are the
promotion of a healthy diet, encouragement of more exercise, and measures to
reduce stress; these practices do a better job of preventing, slowing, and even
reversing heart and other diseases than most drugs and surgical procedures. To
get patients to make the lifestyle changes that appear to be so crucial for
lowering the risk of serious disease, requires practitioners to lavish
attention on them, which means longer, more frequent visits; more focus on
what’s going on in their lives; more effort spent easing anxieties, instilling
healthy attitudes, and getting patients to take responsibility for their own
well-being; and concerted efforts by the practitioner to create emotional bonds
with patients. Through these practices, the practitioner conveys to his
patients his enduring commitment to care for them over time, which imbues the
patients with trust, hope, and a sense of being known.
As
Hippocrates said “It is more important to know what sort of person has a
disease than to know what sort of disease a person has.”
Practitioners
of both biomedicine and alternative/ complementary models emphasize what they
do, and how that makes a difference, with an accompanying explanatory framework
over which practitioners of differing stripes can argue endlessly. Yet beyond
the squabble, lies the fact that health is much more than either biomedicine or
alternative medicine: Health is something onto itself. The allopathic
biomedicine model has privileged surgical procedures and pharmaceuticals, with
doctors doing something or giving something to the patient. Even
with preventive biomedicine, the emphasis is on the doctor issuing the
right set of recommendations – the right intervention – that will make a
difference. The biomedicine model focuses almost exclusively on finding and
evaluating techniques of intervention, rather than on factors like
environments, relationships and meanings, whilst it is more often in the
various modalities of alternative/ complimentary therapies that these latter
aspects are addressed. Just as in the time of the medicine man, shaman and
kahuna, in both of today’s models there are symbols of authority (white coat,
diplomas, prescription pad) and ritual (supplication, diagnosis, prescription
and the power of suggestion from authority).
Generally,
people that DON’T believe in the treatment that they are getting, DON’T do as
well. If they don’t think it’ll make a difference, usually the effect of any
intervention is diminished. Understanding how people come to accept a
particular medical system is an interesting area to study. As decades of
research in medical anthropology has shown, patients need to buy into the local
treatment system for them even to want to access it. Medical practitioners
often employ elaborate persuasive processes to heighten and project their
perceived authority and to compellingly substantiate their diagnoses of
patients’ illnesses (and also to later explain away any treatment failures).
Belief in the treatment model and in the practitioner certainly matters, as
does consensual agreement between the practitioner and the patient as to what
is to be expected in the individual’s healing.
THE PLACEBO
RESPONSE: EVOKING THE INTERNAL HEALER
Medical
practitioners are part-time magicians, and in accordance with tradition the
doctor manipulates the setting and the stage to achieve ‘white magic’ via
placebo (as opposed to nocebo effect, wherein the patient, not
believing, is not healed by legitimate medicine). (Ivan Illich)
There
is a phenomenon in the healing process whereby a totally inert, sham ‘remedy’ brings
about relief and cure of an afflicted person’s symptoms. This phenomenon is so
statistically robust, that – as repeatedly determined in double blind control
tests – it accounts for 30-50% cure rates. The name given to this function is
the placebo response, and so reliable is it that pharmaceutical
companies must control for it and prove that their products have significant
curative potency above and beyond the placebo response to qualify for licensing
and commercialization of their products.
Dr. Henry K. Beecher, an American anesthetist during World War II, is
considered by many to be the father of contemporary placebo research. Dr.
Beecher assisted in surgery during the Allied campaigns in North Africa, Italy
and France. In one battle his battalion was cut off from any supplies, with 225
soldiers having severe wounds, which caused a morphine shortage. In order to
ration the morphine, Dr. Beecher went up to each soldier and asked how intense
the pain was felt by the soldier. To Beecher’s surprise, although these
soldiers had shrapnel and bullet wounds, three-quarters of them perceived so
little pain that they did not ask for pain relief. Further, it wasn’t that the soldiers were in a state of shock, nor unable to
feel pain; indeed, they complained when the IV lines were inserted. Beecher was
surprised because – compared to his experience in civilian practice – civilian patients with
equivalent injuries had reported much greater pain than these wounded soldiers.
Later, Beecher came to understand that the difference between the two groups as
to apparent pain perception wasn’t because of the mental strength of the
soldiers, but rather it was due to the context of the pain.
The meaning attached to the injuries by the respective members
of the two groups affected their perceptions. To the soldier, the wound meant surviving the
battlefield and returning home, while the injured civilian often faced the
personal expense of major surgery, loss of income, diminishment of activities,
and many other negative consequences. These added stresses amplified the civilian’s
pain, whereas the soldiers’ thoughts filtered out most of the pain.
Ultimately Dr. Beecher concluded that the reality of the wound was not the same
as the perception of associated pain; that drugs work because they are able to
connect to receptors in the brain; and that placebos work because rather than
an active drug having entered the body from outside, the patient’s own body has
created the necessary curative chemicals on its own.
As a result of his continuing research, by 1955 Beecher was admonishing other researchers to
pay attention to the negative aspects of intention, expressed as a ‘nocebo’
effect, saying:
“Not only do placebos produce beneficial results, but like other
therapeutic agents they have associated toxic effects. In consideration of 35
different toxic effects of placebos that we had observed in various of our
studies, there is a sizable incidence of such effects attributable to the
placebo.”
Over the ensuing 50+
years, the fascinating field of placebo research has revealed that the body’s
resilience repertoire contains a powerful self-healing network that can produce
natural analgesics such as dopamine to reduce pain and inflammation, and other
endogenous neurochemicals that reduce production of stress chemicals like
cortisol and insulin and even naturally regulate blood pressure and the tremors
of Parkinson’s disease. Jumpstarting this self-healing network often requires
nothing more or less than a belief that one is receiving effective treatment –
in the form of a pill, a capsule, talk therapy, E-M frequency, injection, IV,
or acupuncture needle. The activation of this self-healing network is what is
really meant in reference to the placebo response. Though inert in themselves,
placebos act as passwords between the domain of the mind and the domain of the
body, enabling the expectation of healing to be in turn translated into
cascades of neurotransmitters and altered patterns of brain activity that
engender health.
Over the years, perhaps one of the strangest
situations involving the placebo effect was that experienced by the London,
England anesthesiologist, Dr. Albert Mason. One of Mason’s jobs
was delivering babies; he wanted to explore different ways to relieve the pain
of his patients, so he began to practice medical hypnosis, and delivered 26
babies through hypnosis alone. The hospital staff became very intrigued by this
and allowed Mason to attempt hypnosis to cure patients with all kinds of
aliments. Mason found that his hypnosis was also very effective in curing
warts.
One day a 15 year old boy arrived covered with
millions of warts all over his body which made his skin look like an elephant’s
hide. The hospital doctors were unable to help the patient, and Mason asked if
they had attempted hypnosis. The head surgeon sarcastically remarked, “Why
don’t you try,” which is exactly what he did. He hypnotized the boy and
told him that his left arm would be clear of the warts. After a week the boy came
back to the hospital and his entire left arm was clear. Mason took the lad to the surgeon and showed him the
arm, and said to him, “Well, I told you the warts would go.” According to
Mason, the surgeon said “This is not warts you bloody fool, this is a condition
called congenital ichthyosiform erythroderma. It’s congenital and
incurable.” Mason believes that this was the point when he lost his ability to heal
congential ichthyosis, because after that meeting he was never able to cure
another patient of that disease.
Mason eventually quit his position at the
hospital and later became a psychiatrist. He eventually came to believe that
the placebo effect was able to work both ways during his hypnosis. He could
introduce the idea to his patients that they would get better, but when he was
himself informed that the disease was “incurable” he subconsciously became
unable to perform hypnosis. He has
written many papers and reviews but is perhaps best known for his paper on
hypnotism in which he suggests that the influence of the hypnotist on the
patient requires a shared delusional system, a folie a deux.
- - - - - -
Scientists have
recognized for some time that people suffering from depression often experience
a substantial reduction in symptoms when given a placebo. In fact, this
observation has led some researchers to propose that up to 75 percent of the
apparent efficacy of antidepressant medicine may actually be attributable to
the placebo effect. People want/ hope to be relieved of their depression
suffering, and submit to the healer’s ritual. The results of a 2002 study (2) by a team of researchers led by Dr. Andrew Leuchter at the Psychiatry and Biobehavioural Sciences Dept., UCLA noted that depressed patients responding to placebo treatment
exhibit a change in brain function, but one that differs from that seen in
patients who respond to pharmaceuticals.
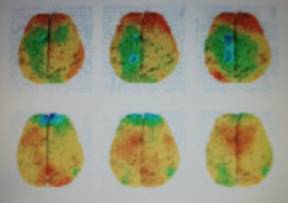
Using
quantitative electroencephalography imaging, the UCLA team studied electrical
activity in the brains of 51 depressed patients receiving either placebo
treatment or active medication. In patients responding favorably to the
placebo, there was increased activity in the prefrontal cortex region of the
patients’ brains. In contrast, those responding to pharmaceutical medication,
exhibited suppressed activity in that area.
The
image shown here illustrates changes in prefrontal cortex activity over time in
the placebo responder group (top row) and in the medication responder
group (bottom row): with red indicating an increase in brain activity
and blue-green representing a decrease.
Dr. Leuchter noted
"Both treatments affect prefrontal brain function, but they have distinct
effects and time courses… The results show us that there are different pathways
to improvement for people suffering from depression. Medications are effective,
but there may be other ways to help people get better and if we can identify
what some of the mechanisms are that help people get better with placebo, we
may be able to make treatments more effective.”
[Compilers’ observation: when placebo was administered and the
patient’s Internal Healer was evoked, the brain’s frontal cortex (the
organizing, rational Executive function) was activated, rather than
being suppressed by exogenous pharmaceuticals.]
Perhaps
rather than considering the placebo response solely as a phenomenon of
belief-constructs, it would be closer to the mark to consider the process as
one of asking for – and receiving from the therapist – permission to heal one’s
own body (or mind). Perhaps the patient simply gains sufficient assurance
from the therapist’s attempts to treat him, that he can consider himself to be
sufficiently worthy to proceed with activation of his Internal Healer.
Evidence-based
biomedicine has worked hard to put a great deal of distance between itself and
the “magical side” of the art of medicine, but the controversy over the placebo
response implies that it is hard to entirely escape this ‘magical side’. The
placebo effect smacks of faith healing and other practices that look blatantly
superstitious to science-based practitioners. The other side of the coin – the
so-called nocebo effect – tilts all too closely in many minds to sorcery, black
magic and witchcraft. When searching for diagnostic techniques and treatments
for the diseases and organic problems of their patients, practitioners of
evidence-based biomedicine are not deeply concerned with what meaning a
patient perceives in how the illness began or how it’s being treated – unlike
the primary concerns of shamans, curanderos and healers of other medical
traditions across millennia of time.
The
science-based biomedical model with its highly rational approach to diagnosing
and curing diseases and in its emphasis on biological reductionism has
instilled in its practitioners a cultural “blinder” or bias against the
holistic approach. Because of the personal and cultural beliefs of patients and
their search for the meaning of their suffering, many patients resist reducing
their maladies to physiological malfunctions, and they appreciate practitioners
willing to pay attention to their own narrative of the illness and its meaning
to themselves. This narrative may not be rational from the perspective of an
evidence-based doctor – especially if there are significant cultural
differences between patient and doctor – but the narrative may be very
logical when viewed within another framework, one with an alternate set of
basic assumptions regarding the nature of reality. Different logics, after all,
are based on different assumptions, and what isn’t logical in one context may
be very logical in another. The meaning narrative – when accepted by
sufferer and other – may precede a positive response to a symbolic placebo –
perhaps some sacrament, or transcendental contact with the sacred, or a ritual
that evokes faith in something beyond the ordinary – and opens the conduit
through which the Internal Healer may emerge. Sensitive responses by healers to
the common human desire for meaning may trigger the patient’s Internal Healer
in ways that external interventions based on evidence-based medicine couldn’t.
CAVEAT:
Dr. Dean Ornish of UCSF notes, “75 percent of the $2.6
trillion the U.S. spent on health care was for treating chronic diseases that,
to a large degree, can be prevented or reversed through lifestyle change”.
Thus notwithstanding our earlier observations and pragmatically bearing in mind
systemic revenue interests, there is a recognizable conflict of interest
inherent in the illness industry. It just wouldn’t make sense to expect
physicians – who, after all, have spent hundreds of thousands of dollars and a
decade of their lives becoming trained in anatomy, biochemistry, high-tech
diagnosis and pharmacology, etc – to spend long blocks of time bonding with
patients and helping them empower themselves through becoming more self-reliant
on their internal healing mechanisms, thereby weaning themselves off exogenous,
cross-indicating pharmaceuticals. Professionals in a medical system that
successfully guided patients toward healthier lifestyles would almost certainly
experience dramatically reduced cash flows. Also, the pharmaceutical business is, after
all, a business, and companies are supposed to boost sales and returns to
shareholders, so it is common knowledge that drugmakers make sure that the
researchers and doctors who extol the benefits of their medications are well
compensated. Who, then, aside from the
patients, has any tangible incentive to make changes that would remove monies
from the health care system?
REPORTS FROM TO-DAYS
EXPLORERS OF LIFE’S INTERNAL HEALING MECHANISMS
F Irving Kirsch - lecturer in
medicine at the Harvard Medical School and the Beth Israel Deaconess Medical
Center), and Associate Director of the Harvard Program in Placebo Studies - PiPs*
As an outgrowth of his interest in the placebo
effect, Professor Kirsch performed extensive analyses of the real effectiveness
of antidepressants. His studies were primarily meta-analyses, in which the
results of previously conducted clinical trials were aggregated and analyzed
statistically. His first meta-analysis – limited to published clinical trials –
was aimed at assessing the size of the placebo effect in the treatment of
depression: the results not only showed a very sizable placebo effect, but also
indicated that actual effects of the active drug itself was surprisingly small.
This naturally led to considerable controvery, whereupon Kirsch shifted his
focus to evaluating the antidepressant drug effect through obtaining files from
the U.S. Food and Drug Administration (FDA) containing data from trials that
had not been previously published, as well as those from
published trials.
[It should be here noted that to gain FDA
licensing approval to market their products, pharmaceutical companies are
required to produce trial results showing that a product performs better than
placebo; the kicker is that they can run x number of trials, yet
only submit those trial results showing favorable results.]
Kirsch’s meta-analyses of the FDA data showed
that the difference between antidepressant drugs and placebos is not clinically
significant according to the criteria used by the National Institute for Health
and Clinical Excellence (NICE), which establishes treatment guidelines for the
National Health Service (NHS) in the United Kingdom.
As a result of his analyses, Kirsch developed the
response expectancy theory, which is based on the idea that what people
experience depends partly on what they expect to experience. According to
Kirsch, this is a major part of the process that lies behind the placebo effect
and also hypnosis. The theory is supported by research showing that both
subjective and physiological responses can be altered by changing people’s
expectancies, and it has been applied to better understanding pain, depression,
anxiety disorders, asthma, addictions, and psychogenic illnesses.
Kirsch argues (3) that the widely-held theory that depression is caused by
a chemical imbalance is wrong:
"It now seems beyond question that the traditional account of
depression as a chemical imbalance in the brain is simply wrong … and the kinds
of effects you see in the brain when people respond to a placebo depends on the
condition you’re supposed to be treating. So if you take a placebo analgesic,
you get reductions in activity in the brain’s pain matrix. If you take a
placebo antidepressant, you get changes in brain activity in areas related to
depression.”
In
his own placebo experiments, Kirsch prepped volunteers by informing them that
placebo effects work via classical conditioning, like Pavlov’s dogs being
trained to salivate at the sound of a bell. He reported “people all over the world respond to the act of taking a pill when
informed of the existence of prior successful treatments. People come to expect
and believe that they’re going to get better if they take medication. The whole
process of going to a physician and being treated reinforces this belief, and that
constitutes the basic aspects of classical conditioning. Eventually, the pill
alone is enough to produce a placebo effect, whether it contains an active drug
or not.”
Kirsch
also indicated that “direct-to-consumer drug
advertising also plays a role; e.g. it has been proven in meta-analyses of
anti-depressants that none of them perform better than placebos, yet in the
anti-depressant market in America, when you open a magazine, the good-looking
jock playing with puppies in the sun is the formerly depressed patient on
Zoloft. One thing that’s clear is that the placebo effect of antidepressants
has gotten stronger over the years as these drugs have been more widely
accepted, touted, and advertised… We have the capacity for healing physical
conditions through psychological means.
There
used to be an ethical concern in the medical profession as to a doctor
presenting a placebo that he knew was inert, to a patient who in effect had been
deceived into believing the pill was medically active. According to Kirsch (3) “that no longer has to be a concern, since now we know that the placebo
effect still works even when people know they’re taking placebos. That’s one of the nice things
we’ve learned from these studies. Plus, there’s an ethical problem when you
keep secret the fact that you’re giving someone a drug that barely works –
especially when the drug has harmful effects as well… These studies suggest
that in the brain, belief is a two-tiered process: one that knows there’s
nothing in this pill, and another that knows that a placebo can be an effective
treatment. It’s as if the brain can entertain two different notions of the
effectiveness of a pill at once… these are not contradictory notions. I believe
in both. I know that this pill does not contain a physically active ingredient,
and I also understand the conditioning process. I know that the placebo effect
is real, so I understand that this inert pill might help trigger that healing
response within me. We need to recognize and understand that patients are
active agents in their treatment, not passive. The placebo effect does not come
from the pill. It comes from the patient.”
Quotes
from Irving Kirsch’s landmark book - The Emperor's New Drugs: Exploding the
Antidepressant Myth (4)
“Depression is a serious problem, but drugs are not the answer. In
the long run, psychotherapy is both cheaper and more effective, even for very serious
levels of depression. Physical exercise and self-help books based on CBT can
also be useful, either alone or in combination with therapy. Reducing social
and economic inequality would also reduce the incidence of depression.”
“Our analyses of the FDA data showed relatively little difference
between the effects of antidepressants and the effects of placebos. Indeed, the
effects were so small that they did not qualify as clinically significant. The
drug companies knew how small the effect of their medications were compared to placebos,
and so did the FDA and other regulatory agencies. The companies found various
ways to make the data seem more favorable to their products, and the FDA helped
them keep their negative data secret. In fact, in some instances, the FDA urged
the companies to keep negative data hidden, even when the companies wanted to
reveal them. My colleagues and I hadn't really discovered anything new. We had
merely revealed their 'dirty little secret'.”
“Physicians do not systematically prescribe placebos to their
patients. Hence they have no way of comparing the effects of the drugs they
prescribe to placebos. When they prescribe a treatment and it works, their
natural tendency is to attribute the cure to the treatment. But there are thousands
of treatments that have worked in clinical practice throughout history.
Powdered stone worked. So did lizard's blood, and crocodile dung, and pig's
teeth and dolphin's genitalia and frog's sperm. Patients have been given just
about every ingestible - though often indigestible - substance imaginable. They
have been 'purged, puked, poisoned, sweated, and shocked', and if these
treatments did not kill them, they may have made them better.”
“Like antidepressants, a substantial part of the benefit of psychotherapy
depends on a placebo effect, or as Dan Moerman calls it, the meaning
response. At least part of the improvement that is produced by these
treatments is due to the relationship between the therapist and the client and
to the client's expectancy of getting better. That is a problem for
antidepressant treatment. It is a problem because drugs are supposed to work
because of their chemistry, not because of the psychological factors. But it is
not a problem for psychotherapy. Psychotherapists are trained to provide a warm
and caring environment in which therapeutic change can take place. Their
intention is to replace the hopelessness of depression with a sense of hope and
faith in the future. These tasks are part of the essence of psychotherapy. The fact
that psychotherapy can mobilize the meaning response - and that it can do so
without deception - is one of its strengths, not one of its weaknesses. Because
hopelessness is a fundamental characteristic of depression, instilling hope is
a specific treatment for it. Invoking the meaning response is essential for the
effective treatment of depression, and the best treatments are those that can
do this most effectively and that can do so without deception.”
[See footnote (4) for link to further Kirsch quotes]
F Ted J. Kaptchuk - Associate
Director of the Harvard Program in Placebo Studies - PiPs*
From “Placebo studies and ritual theory: a
comparative analysis of Navajo, acupuncture and biomedical healing” by Ted J. Kaptchuk (5)
“Taken as a whole, the study of placebos illuminates theory in
several concrete ways. Minimally what has been found includes:
·
Rituals have
neurobiological correlates. This suggests that patient improvement is not only
report bias or desire to please the healer but represents changes in
neurobiology. Specific areas of the brain are activated and specific
neurotransmitters and immune markers may be released.
·
Biomedical
treatment with powerful medications has a ritual component that is clinically
significant.
·
As with
pharmaceuticals, each type of ritual, for example, fake needles versus fake
pills, has a unique outcome.
·
Components
of rituals can be disaggregated and incrementally combined in a manner
analogous to a dose response. For example, adjusting components of a ritual
could make it more or less persuasive.
·
When
engaged in a ritual, patients do not abandon practical sensibilities. Hope,
openness and positive expectancy are tempered with uncertainty and realistic
assessment.
·
Different
healers can have different effects on patients even when they perform an
identical, prospectively-defined, precise, scripted interaction.
“At a minimum, healing rituals provide an opportunity to reshape
and recalibrate selective attention. In a more expanded model, rituals trigger
specific neurobiological pathways that specifically modulate bodily sensations,
symptoms and emotions.
It seems that if the mind can be persuaded, the body can sometimes
act accordingly. Placebo studies may be one avenue to connect biology of
healing with a social science of ritual. Both placebo and ritual effects are
examples of how environmental cues and learning processes activate
psychobiological mechanisms of healing.
In conclusion, for biomedicine the ‘placebo
effect’ has been primarily of interest as a non-specific process that needs to
be controlled. In contrast, for ritual theory, the placebo effect is the
specific effect of a healing ritual. Combining placebo studies with ritual
theory can help provide a conceptual shift to counteract the ideological
devaluation of ritual in biomedicine. The linkage of ritual theory and placebo
studies can expand the discourse of both fields.” (5)
From ‘‘Maybe I Made Up the Whole Thing’’: Placebos and
Patients’ Experiences in a Randomized Controlled Trial” (6):
“Interviews of the 12 qualitative subjects who underwent
and completed placebo treatment were transcribed. We found that patients:
(1) were persistently concerned with whether they were receiving
placebo or genuine treatment;
(2) almost never endorsed ‘‘expectation’’ of improvement but spoke
of ‘‘hope’’ instead and frequently reported despair;
(3) almost all reported improvement ranging from dramatic
psychosocial changes to unambiguous, progressive symptom improvement to
tentative impressions of benefit; and
(4) often worried whether their improvement was due to normal
fluctuations or placebo effects.
The placebo treatment was a problematic perturbation that provided
an opportunity to reconstruct the experiences of the fluctuations of their illness
and how it disrupted their everyday life. Immersion in this RCT was a
co-mingling of enactment, embodiment and interpretation involving ritual
performance and evocative symbols, shifts in bodily sensations, symptoms, mood,
daily life behaviors, and social interactions, all accompanied by self-scrutiny
and re-appraisal. The placebo effect involved a spectrum of factors and any
single theory of placebo – e.g. expectancy, hope, conditioning, anxiety
reduction, report bias, symbolic work, narrative and embodiment – provides an
inadequate model to explain its salubrious benefits.”
[Compilers’
observations as to the four Kaptchuk et al findings]
1 – uncertainty gives rise to the patient’s co-effort vs.
dependency state
2 – hope instead of expectation introduces the
‘Doubt’ aspect; Doubt opens the patient’s ‘self-permission to heal’ aperture
3 – attention from another in the treatment ritual
stimulates the perception by the patient’s of his ‘worthiness-to-improve’ on
various levels
4 – again, doubt allows the ‘permission>self-cure process’ to
cycle
“The emergent
neuroscience hypothesis of ‘prospection’ provides another way of thinking about
our findings concerning ‘expectation’ and ‘hope’. ‘Prospection’ proposes that
people constantly build simulations of the future in their minds to explore
different future scenarios. This multiplex theater operates as a stage
or representational space whereby simulations of the future can be
constructed and explored. A proposed detail of this constructional space is
that it allows a representation of current reality and also secondary
representations that explore future possibilities’’ (Buckner 2007). From this
point of view, our patients are seen to have engaged in a dynamic process that
entertained multiple possibilities of the future (and even the present).
Prospection allows for such multiple possibilities, which could include
improvement, worsening and little change. Hope seems aligned to this notion of
prospection and represents openness to multiple outcomes including
amelioration.
Still another, more anthropological rubric for the examination of
‘expectation’ and ‘hope’ is the concept of ‘subjunctivity’ of illness
narratives, a concept that medical anthropology borrowed from the field of
literary criticism. In telling (or thinking) the story of their illnesses,
especially chronic illnesses, individuals are often careful to indicate some
uncertainty, if not frank hope, as to the anticipated future course. Theorists
of ritual have noted that this subjunctive ‘as if’ framework can actually pull
someone into a deeper level of participation and somehow ‘make the illusion the
reality’
… what began as an ‘‘as if’’ subjunctive interpretation of
experience later became the premise for a construction of a healing encounter
built on enactment, embodiment and interpretation – ultimately experienced as
healing…
The context of an acupuncture regime might not generalize to
patients who undergo more
familiar, conventional medication pill therapy. Besides having potentially
expansive psychological dimensions, placebo acupuncture involves highly focused
directed attention that is enveloped by unique kinds of apprehension,
anxiety and trust and autonomic arousal, more akin to what happens in a
multi-sensory healing ritual than the more medical behavior of simply taking a
pill” (6)
From Placebos
without Deception: A Randomized Controlled Trial in Irritable Bowel Syndrome: (7)
“Patients were randomized to either open-label placebo
pills presented as “placebo pills made of an inert substance, like sugar pills,
that have been shown in clinical studies to produce significant improvement in
IBS symptoms through mind-body self-healing processes” or
no-treatment controls with the same quality of interaction with providers.
Open-label placebo produced significantly higher mean global improvement scores
at both 11-day midpoint and at 21-day endpoint…. Placebos administered without deception may be an effective
treatment for IBS.”
[Compilers’
observation: Patients were told that the pills do work, and
that clinical studies had shown this. They were even told how they work
– "through mind-body self-healing process". This is for most people
an explanation at least as comprehensible and rational as being told that they
work by blocking the potassium channel or selectively inhibiting serotonin
re-uptake.]
F Fabrizio Benedetti, M.D. - Professor of Physiology and Neuroscience, University of Turin - PiPs*
“Any medical treatment is surrounded
by a psychosocial context that affects the therapeutic outcome. If we want to
study this psychosocial context, we need to eliminate the specific action of a
therapy and to simulate a context that is similar in all respects to that of a
real treatment. To do this, a sham treatment (the placebo) is given, but the
patient believes it is effective and expects a clinical improvement. The
placebo effect, or response, is the outcome after the sham treatment.
Therefore, it is important to emphasize that the study of the placebo effect is
the study of the psychosocial context around the patient.
The placebo effect is a
psychobiological phenomenon that can be attributable to different mechanisms,
including expectation of clinical improvement and Pavlovian conditioning. Thus,
we have to look for different mechanisms in different conditions, because there
is not a single placebo effect but many. So far, most of the neurobiological
mechanisms underlying this complex phenomenon have been studied in the field of
pain and analgesia, although recent investigations have successfully been
performed in the immune system, motor disorders, and depression. Overall, the
placebo effect appears to be a very good model to understand how a complex
mental activity, such as expectancy, interacts with different neuronal
systems.” (8)
Nocebo:
(From Guardian UK article)
… Until recently, we knew very little about how
the nocebo effect works. Now, however, a number of scientists are beginning to
make headway. A study in February led by Oxford's Professor Irene Tracey showed
that when volunteers feel nocebo pain, corresponding brain activity is
detectable in an MRI scanner. This shows that, at the neurological level at
least, these volunteers really are responding to actual, non-imaginary, pain.
Fabrizio Benedetti and his colleagues have managed to determine one of the
neurochemicals responsible for converting the expectation of pain into this
genuine pain perception. The chemical is called cholecystokinin and
carries messages between nerve cells. When drugs are used to block
cholecystokinin from functioning, patients feel no nocebo pain, despite being
just as anxious.
The findings of Benedetti and Tracey not only
offer the first glimpses into the neurology underlying the nocebo effect, but
also have very real medical implications. Benedetti's work on blocking
cholecystokinin could pave the way for techniques that remove nocebo outcomes
from medical procedures, as well as hinting at more general treatments for both
pain and anxiety. The findings of Tracey's team carry startling implications
for the way we practise modern medicine. By monitoring pain levels in
volunteers who had been given a strong opioid painkiller, they found that
telling a volunteer the drug had now worn off was enough for a person's pain to
return to the levels it was at before they were given the drug. This indicates
that a patient's negative expectations have the power to undermine the
effectiveness of a treatment, and suggests that doctors would do well to treat
the beliefs of their patients, not just their physical symptoms…. (9)
F Tor D. Wager
(Professor of psychology at the University of Colorado)
Wager’s specialty is neuroscience and brain imaging,
but his passion is the placebo effect – a phenomenon being studied by
researchers in many corners of science. He has written roughly a dozen scientific papers on placebo effects,
including a 2007 study linking pain-related effects to parts of the brain that
process opium or heroin (which may help explain why many placebos are
temporary) – and concluded that “Placebo-induced
expectancies of pain relief have been shown to decrease pain in a manner
reversible by opioid antagonists, but little is known about the central brain
mechanisms of opioid release during placebo treatment.”
For
Wager, the issue of placebo effects entails a deep question, tied to his
childhood religion (Christian Science) and the way he sees the world. Through
his various experiments he discovered that the brain creates the desired chemicals
when a placebo is introduced. In one experiment Wager placed a heating pad on
the test subject’s arm. This caused the subject discomfort, which Wager stated
would go away when he put a pain relief ointment on the subject’s skin. Rather
than doing so, Wager used the equivalent of Vaseline. The moment the placebo
was introduced, the subject was given a brain scan. Wager discovered that the
temporal lobes became excited and then they activated the limbic system, which
is the main producer of opioids…. Wager concluded that the brain can be tricked
into creating chemicals that it wouldn’t normally produce. Wager has done
further experiments with morphine that have allowed patients to be slowly
weaned off a morphine addiction by giving them the basic equivalent of a sugar
pill. “What is the placebo
effect? Well, it’s not some weird magical thing that just kind of happened out
of the blue. I think it’s connected to systems that generate emotional
responses. It’s a window into ways in which psychological factors can affect
brain and body factors that are related to health.” (Source - NY Times)
F Dan Moerman, Phd. – Anthropologist, Department of Behavioral Sciences, University of
Michigan-Dearborn, USA
- PiPs*
(Key
points: Paper entitled “Deconstructing the Placebo Effect and Finding the
Meaning Response” co-published by Daniel E. Moerman, PhD, and Wayne B. Jonas, MD (10)
·
The one thing of which we can be absolutely certain is that placebos do
not cause placebo effects. Placebos are inert and don’t cause anything.
·
Ironically, although
placebos clearly cannot do anything themselves, their meaning can.
·
We define the meaning
response as the physiologic or psychological effects of meaning
in the origins or treatment of illness; meaning responses elicited after the
use of inert or sham treatment can be called the “placebo effect” when they are
desirable and the “nocebo effect” when they are undesirable.
·
Insofar as medicine is meaningful, it can affect patients, and it can
affect the outcome of treatment. Most elements of medicine are meaningful,
even if practitioners do not intend them to be so. The physician’s costume (the
white coat with stethoscope hanging out of the pocket), manner (enthusiastic or
not), style (therapeutic or experimental), and language, are all meaningful
and can be shown to affect the outcome; indeed, we argue that both diagnosis
and prognosis can be important forms of treatment.
·
Meaning Can Have Substantial Physiologic Action: Placebo analgesia can
elicit the production of endogenous opiates. Analgesia elicited with an
injection of saline solution can be reversed with the opiate antagonist
naloxone and enhanced with the opiate agonist proglumide. Likewise, acupuncture
analgesia can be reversed with naloxone in animals and people.
To
say that a treatment such as acupuncture “isn’t better than placebo” does not
mean that it does nothing.
·
Meaning and Surgery: The classic example of the meaningful effects of surgery
comes from two studies of ligation of the bilateral internal mammary arteries
as a treatment for angina. Patients receiving sham surgery did as well – with
80% of patients substantially improving – as those receiving the active
procedure in the trials or in general practice. Although the studies were
small, the procedure was no longer performed after these reports were
published. Of note, these effectiveness rates (and those reported by the
proponents of the procedure at the time) are much the same as those achieved by
contemporary treatments such as coronary artery bypass or beta-blockers.
·
Surgery is particularly meaningful: Surgeons are among the elite of
medical practitioners; the shedding of blood is inevitably meaningful in and of
itself. In addition, surgical procedures usually have compelling rational
explanations, which drug treatments often do not. The logic of arthroscopic
surgery (“we will clean up a messy joint”) is much more sensible and
understandable (and even effective, especially for people in a culture rich in
machines and tools, than is the logic of non-steroidal anti-inflammatory drugs
(which “inhibit the production of prostaglandins which are involved in the
inflammatory process,” something no one would ever tell a patient). Surgery
clearly induces a profound meaning response in modern medical practice.
·
MEANING, CULTURE, AND MEDICINE: Anthropologists
understand cultures as complex webs of meaning, rich skeins of connected
understandings, metaphors, and signs. Insofar as 1) meaning has biological
consequence and 2) meanings vary across cultures, we can anticipate that
biology will differ in different places, not because of genetics but because of
these entangled ideas; we can anticipate what Margaret Lock has called “local
biologies”; Lock has shown dramatic cross-cultural variation in the existence
and experience of “menopause”. Moreover, Phillips has shown that “Chinese
Americans, but not whites, die significantly earlier than normal (1.3 to 4.9
yr) if they have a combination of disease and birth year which Chinese
astrology and medicine consider ill fated”. Among Chinese Americans whose
deaths were attributed to lymphatic cancer (n= 3041), those who were
born in “Earth years” – and consequently were deemed by Chinese medical theory
to be especially susceptible to diseases involving lumps, nodules, or tumors –
had an average age at death of 59.7 years. In contrast, among those born in
other years, age at death of Chinese Americans with lymphatic cancer was 63.6
years – nearly 4 years longer. Similar differences were also found for various
other serious diseases. No such differences were evident in a large series of
“whites” that died of similar causes in the same period. The intensity of the
effect was shown to be correlated with “the strength of commitment to
traditional Chinese culture.” These differences in longevity (up to 6% or 7%
difference in length of life!) are not due to having Chinese genes but to
having Chinese ideas, to knowing the world in Chinese ways. The effects of
meaning on health and disease are not restricted to placebos or brand names but
permeate life.
·
CONCLUSIONS:
Practitioners
can benefit clinically by conceptualizing this issue in terms of the meaning
response rather than the placebo effect. Placebos are inert. You can’t do
anything about them. For human beings, meaning is everything that
placebos are not, richly alive and powerful. However, we know little of this
power, although all clinicians have experienced it.
One
reason we are so ignorant is that – by focusing on placebos – we constantly
have to address the moral and ethical issues of prescribing inert treatments,
of lying, and the like. It seems possible to evade the entire issue by simply
avoiding placebos. One cannot, however, avoid meaning while engaging human
beings. Even the most distant objects – the planet Venus, the stars in the
constellation Orion – are meaningful to us, as well as to others.
Yet,
a huge puzzle remains: Obviously the meaning response is of great value
to the sick and the lame. For example, eliciting the meaning response requires
remarkably little effort (“You will be fine, Mr. Smith”). So why doesn’t this
happen all the time? And why can’t you do it to yourself? Psychologist Nicholas
Humphrey has suggested that this conundrum may have evolutionary roots: Healing
has its benefits but also its costs. (For example, relieving pain may encourage
premature activity, which could exacerbate the injury. Moreover, immune
activity is metabolically very demanding on an injured system.) Perhaps only
when a friend, relative, or healer indicates some level of social support (for
example, by performing a ritual) is the individual’s internal economy able to
act. Moreover, as we have clarified, routinized, and rationalized our medicine,
thereby relying on the salicylates and forgetting about the more meaningful
birches, willows, and wintergreen from which they came – in essence, stripping
away Plato’s “charms” – we have impoverished the meaning of our medicine to a
degree that it simply doesn’t work as well as it might any more. Interesting
ideas such as this are impossible to entertain when we discuss placebos; they
spring readily to mind when we talk about meaning. (10)
F Nicholas
Humphrey - evolutionary psychologist; Professor Emeritus, London School of Economics &
Political Science - PiPs*
“Wherever a
capacity for self-cure exists as a latent possibility in principle,
placebos will be found to activate this capacity in practice. It’s true that
the effects may not always be consistent or entirely successful. But they certainly
occur with sufficient regularity and on a sufficient scale to ensure that they
can and do make a highly significant contribution to human health….
Evolutionary
theory suggests that the human capacity to respond to placebos must in the past
have had a major impact on people’s chances of survival and reproduction (as
indeed it does today), which means that it must have been subject to strong
pressure from natural selection. This capacity apparently involves dedicated
pathways linking the brain and the healing systems, which certainly look is if
they have been designed to play this very role…
The human
capacity for responding to placebos is in fact not necessarily adaptive in its
own right (indeed it can sometimes even be maladaptive). Instead, this capacity
is an emergent property of something else that is genuinely adaptive:
namely, a specially designed procedure for ‘economic resource management’ that
is, I believe, one of the key features of the ‘natural health-care service’
which has evolved in ourselves and other animals to help us deal throughout our
lives with repeated bouts of sickness, injury, and other threats to our
well-being…
When the
sickness is self-generated, cure can be achieved simply by switching off whatever
internal process is responsible for generating the symptoms in the first place;
with pain, for example, you may well be able to achieve relief simply by
sending a barrage of nerve signals down your own spinal cord or by releasing a
small amount of endogenous opiate molecules. Similarly, with depression, you
may be able to lift your mood simply by producing some extra seritonin.
However, it
may be a very different story when the sickness involves genuine pathology and
the cure requires extensive repair work or a drawn-out battle against foreign
invaders – as with healing a wound or fighting an infection or cancer…
People’s bodies and minds have a considerable capacity for
curing themselves. Sometimes this capacity for self-cure is not expressed spontaneously,
but can be triggered by the influence of a third party. In such cases,
self-cure is being inhibited until the third-party influence releases it. When
self-cure is inhibited there must be good reason for this under the existing
circumstances; and when inhibition is lifted there must be good reason for this
under the new circumstances. The good reason for inhibiting self-cure must be
that the subject is likely to be better off, for the time being, not being
cured. Either there must be benefits to remaining sick, or there must be costs
to the process of self-cure. The good reason for lifting the inhibition must be
that the subject is now likely to be better off if self-cure goes ahead. Either
the benefits of remaining sick must now be less, or the costs of the process of
self-cure must now be less…
Many of those
conditions from which people seek relief are not in fact defects in themselves
but rather self-generated defenses against another more real defect or
threat. Pain is the most obvious example. Pain is not itself a case of bodily
damage or malfunction – it is an adaptive response to it. The main function of
your feeling pain is to deter you from incurring further injury, and to
encourage you to hole up and rest. Unpleasant as it may be, pain is nonetheless
generally a good thing – not so much a problem as a part of the
solution.
It’s a
similar story with many other nasty symptoms. For example, fever associated
with infection is a way of helping you to fight off the invading bacteria or
viruses. Vomiting serves to rid your body of toxins. And the same for certain
psychological symptoms too. Phobias serve to limit your exposure to potential
dangers. Depression can help bring about a change in your life style. Crying
and tears signal your need for love or care. And so on. Now, just to the extent
that these evolved defenses are indeed defenses against something worse,
it stands to reason that there will be benefits to keeping them in place
and costs to premature cure.
If you don’t
feel pain you’re much more likely to exacerbate an injury; if you have your
bout of influenza controlled by aspirin you may take considerably longer to
recover; if you take Prozac to avoid facing social reality you may end up
repeating the same mistakes, and so on. The moral is: sometimes it really is
good to keep on feeling bad. On the other hand ….
What placebo
treatments do, is to precisely give people reason to hope, albeit that the
reason may in fact be specious. No matter, it works!… Your evolved health-care
management system may sometimes make egregious errors in the allocation
of resources – errors which you can only undo by overriding the system
with a placebo response based on invalid hope…” (11)
F Howard L. Fields, MD, PhD - Professor of
Neurology and Physiology, UCSF - PiPs*
Professor Fields is also
Director of Human Clinical Research, Gallo
Center and the Wheeler
Center for the Neurobiology of Addiction, and he notes how
our brains are powerfully affected by others’ words, body language and tone of
voice – to the extent of reducing the effect of drugs (and reduced need for
them), and – in the case of placebos – when subjects are advised of
‘side-effects’, they tend to get them. He emphasizes that our lives are all
unique (even in the case of identical twins) because of our having learned from
ongoing, personally unique experiences
– including formal and informal education, books, observation and social
environment – all of which give each of us a world-view different from any
others, and because of that, different things affect each person differently.
The
following comments were drawn from Setting
the Stage for Pain - Allegorical Tales from Neuroscience
by Professor Fields: (12)
“Since our subjective experience of self, body, and world is an emergent
property of dynamic networks of coordinated neural activity, the brain must
contain representations of the body, the self (mind), and the external world.
These representations give rise to the ongoing subjective experience of the
individual. Representations are a neural (physical) embodiment of meaning that
is often understood in the context of intention. Intention assumes goals; goals
imply values. A major task of the brain is to make choices between goals, and
this in turn depends on values and predictions of consequences….
The interacting dyad of brain and context is the canvas upon which
"we" continually create ourselves. The brain is the site where
culture and biology interact. It is an interface constrained by the laws of
physics but liberated by imagination and hope.
Rather than passively reproduce images from sensory stimuli, the
brain actively uses these inputs to combine and shape images that are selected
from a potentially large but limited pre-existing file… Each individual will
have a nervous system that is shaped by his or her unique experience. This is
powerfully influenced by language, religion, and other cultural factors. A key point is that this influence is a
two-way street: not only do bodily and environmental factors create central
representations; these representations strongly influence the interpretation of
ongoing experience…
The experience of pain is the result of activating a neural
representation in the brain and is projected in space to the site of tissue
injury. The point is that the pain is generated at a site distant from the
injury but is perceived to be at the injury site due to projection. The pain is
generated in the brain. It is neural and mental. It is physical pain in the
sense that nerve cells and their activity are physical. It is mental pain in
the sense that it is subjectively experienced in what we generally call
the mind… Once one understands and accepts the concept of projection, it
becomes obvious that all pain is mental. Furthermore, what most people call
mental or emotional pain is ontologically identical to what they call organic,
physical, or bodily pain. Once this point is appreciated, many confusing
phenomena, such as the placebo response, somatization, psychologically induced
headache, and analgesia in trance, become less surprising and arcane…
The sensory system is not a passive conduit for transmitting
information about stimuli. The sensory system is active in the context of
goal-directed behaviors and provides data the brain uses to evaluate the
consequences of specific actions. The brain is not passive; it is actively
probing and exploring. At any given time, what the brain ‘perceives’ depends as
much on what questions it is asking and what happened in the past as it does on
what stimuli are presented to it. The modifications that take place can be
thought of as transformations of the meaning of the neural activity produced by
tissue-damaging stimuli.
How could pain transform meaning, and how could meaning transform
pain? There is no doubt that these transformations occur…. By the process of
association, pain can transform the meaning of contextual cues, intentions, and
behaviors. It is no accident that the Latin root of the word "pain"
is punishment. Punishment is a core interpersonal transaction that leads to social
control and the reinforcement of cultural norms. For example, take the dictum
“Honor thy parents”. Parents may inflict pain on their children if they lie,
deliberately break things, or simply act in a defiant manner. Through the
agency of punishment, the (actual or intended) performance of the punished act
acquires new meaning. One could argue that obedience becomes a good because of
its association with the avoidance of pain. The threat of pain can become
incorporated into cultural myths that serve the same purpose as punishment. For
example, in some ideas of hell, physical pain plays a prominent role.
Conversely, pain can transform behaviors in the opposite direction.
You might say that defiance is transformed from disrespect to courage when it
is done in the anticipation of physical punishment. What the parent views as
evil, the child's peers might view as a good. In this case, the concept of
courage (or defiance) requires cultural insights and is usefully informed by
anthropology and/or sociology. Courage is generally thought to be good, but
again, good and bad are not scientific constructs.
… In 1991 Bayer and colleagues examined normal volunteers who had
electrodes placed on their temples. The subjects were told that they would
receive electrical stimulation at increasing intensity and were to report the
level of pain they experienced. The stimulus intensity was signaled by an
intensity gauge that the subject could view and by a tone whose pitch increased
in increments that were parallel with the gauge readings. One hundred subjects were included in the study.
They were divided into five groups and given different instructions. Although no
stimulus was actually delivered (the electrodes were not connected to a power
source), up to 50 percent of subjects reported pain at the electrode site, and
up to 25 percent requested pain medication. This study is very important
because severe pain was elicited in the absence of any stimulation. It
illustrates the power of meaning to influence the pain experience.” (12)
·
From “The Triumph
Of New-Age Medicine” by David H. Freedman - Atlantic Magazine July-Aug 2011
(13)
“Mainstream
medicine uses the placebo effect all the time,” says Ted Kaptchuk, a Harvard
researcher who studies the impact of placebos. “Doctors don’t tell you the drug
they’re giving you is barely better than a placebo. They all spin.” To be
approved by the FDA, a drug has to do better than a placebo in studies – but
most approved drugs do only a little better, and for many drugs the evidence is
mixed. A number of studies have indicated, for example, that most
antidepressants don’t do better than placebos, but patients filled more than
250 million prescriptions for them in 2010. The vast majority of drugs don’t
work in as many as 70 percent of patients, according to an estimate from within
the pharmaceutical industry. One recent study concluded that 85 percent of new
prescription drugs hitting the market are of little or no benefit to patients.
Of
course, whether doctors or alternative practitioners are really ‘lying’ when
they ply patients with drugs or homeopathic remedies is a matter of judgment –
we can’t know how much any individual caregiver believes in these treatments,
although a noteworthy 2008 survey found that about half of U.S. physicians
admit they routinely prescribe treatments they don’t think are likely to be of
direct physical benefit. Regardless, notes Kaptchuk, patients absolutely end up
feeling better, and often testing healthier, when they get these non-effective
treatments, thanks to the placebo effect. “Knowing that you’re getting a
treatment,” he says, “is a critical part of the ritual of seeing any kind of
practitioner.”
Many
studies have proved that sham-treatment rituals can do as well as drugs and
surgery in relieving symptoms of many common and debilitating ailments. A 2002
study found that sham knee surgery involving an incision but nothing else did
as much to relieve arthritis as the standard real procedure, and a 2009 study
found that the same was true of a common back operation for osteoporosis. A
2008 British Medical Journal study by Kaptchuk and several colleagues
showed that patients receiving sham treatment for irritable bowel syndrome –
which is one of the 10 disorders that most frequently bring patients to doctors
and which has been estimated to cost the U.S. up to $30 billion a year – did as
well as patients typically do on the standard drug for the disorder. A 2001
study showed that in patients suffering from Parkinson’s disease, a condition
marked by the brain’s diminished ability to produce dopamine, a placebo
treatment caused dopamine production to surge.
A
German Medical Association study this year found that 59 percent of patients
with stomach discomfort were helped by sham treatments. “Placebos have a
stronger impact and are more complex than we realized,” German Medical
Association Director Christoph Fuchs stated upon the study’s release. “They are
hugely important in medicine today.”
Studies
by Kaptchuk and others have even shown that patients still get a beneficial
placebo effect when practitioners are honest but optimistic with patients about
the placebo – saying something along the lines of “We know of no reason why
this should work, yet it seems to work with many patients.” (13)
·
Here is a three
minute video re the curious phenomenon
where taking a substance that has no known medicinal value makes us feel
better. This video takes a look at the many strange effects of placebos, as
well as the effects of our perceptions on their efficacy: pill size or number of
pills swallowed, pill colour, packaging, delivery method (pills versus
injections, for example), our symptoms, where in the world we live ... and yes,
it's possible to become addicted to placebos!
·
http://richarddawkins.net/videos/3484-richard-dawkins-interviews-nicholas-humphrey 4 parts
[includes an interesting reference to Fabrizio Bennedette
- who has earlier performed conditioning experiments on others that boosted the
efficacy of placebo from 30% to 90%], had also applied ‘placebo’ to himself –
cutting his arm and then administering an inert injection into himself… and it
worked to dispel his pain. In this case he wasn’t ‘tricked’ by an authority;
the placebo worked because he himself knew that placebos work, so it
worked.]
·
An excellent article by Steve
Silberman entitled “Placebos Are Getting More Effective. Drugmakers Are Desperate
to Know Why”, with references to Tor Wager, Ted Kaptchuk and Fabrizio Benedetti, at
http://www.wired.com/medtech/drugs/magazine/17-09/ff_placebo_effect?currentPage=all
·
An American study of 8,000 people who had been treated for depression
found that a quarter of them were not clinically sick, but had just undergone a
normal life event such as bereavement.
Their symptoms, it said, should be left to pass
naturally (that, of course, would be a blow to the drug manufacturers, who
profit so handsomely from the mass consumption of their mind-numbing
chemicals). One leading expert, Randolph Nesse, a
psychiatry professor at Michigan University, argues that mild forms of depression
are beneficial, often interjecting into our lives to tell us to stop what we
are doing and reconsider. This can help when something awful happens to us,
such as a job loss or relationship break-up, when it makes sense to slow down
to grieve, reassess and make changes. [But instead, we live in a world that
tells us that when we feel out of sorts we need a pill to recover.] (from a Dec 2010 Daily Mail UK article
entitled “Will we ever wake up to the deadly risks
of happy pills?”
[Compilers’ observation: Consider
Professor Nesse’s comments in relation to the foregoing findings concerning
invocation of the endogenous Healing Response through ‘rituals’ and ‘empathy’: Sometimes a person just needs a
little recogition when suffering the let-down associated with bereavement,
estrangement, or failure – and human empathy, not stupification, is what is
really needed.]
·
HUNA - The essence of this ancient
Polynesian-Hawaiian teaching is that the human being is made up of three
Selves, or minds. These can most easily be understood as the Lower Self (the
administrator of all organic functions and location of the sub-conscience
mind); the Middle Self (the daily conscience mind and world-senser); and the
Higher Self (the evolutionary super-entity). Huna taught that each of these
tripartite aspects has its own discrete role to perform in each individual’s
life, health and happiness – which can only come about as a result of the
proper integration, blending, and harmonization of the Three Selves. As an
example, the Middle Self can’t tinker with the fundamental drives or organic
workings of the Lower Self, but can only try to influence the Lower Self
(through logic, prayer or shamanic intercession) to make an appeal to the
Higher Self for redirection (permission) to implement restorative adjustments.
Concerning the imagination-will-body triangle, consider the
placebo effect. Years ago, if a patient's symptoms could not be given a
diagnostic label, the doctor would say, "It's just your imagination."
As you know a certain percentage of the population is cured by taking a
medicine that has no curative property; it is just a pill with nothing in it.
How do these people get well? It seems to me that their will to get well
directs their imagination which on its own, in turn, influences body chemistry.
I suppose that those people who are healed by a placebo have a closer connection,
maybe a direct line from the will to the imagination and body.
Which brings up the point that in identical situations, one
person may die and another not die. Now I think that maybe in one the
connection of will (in this case the will to die) to imagination and body was
stronger than in the other. (Laura
Huxley)
Like a celestial chaperon, the placebo leads us through the
uncharted passageways of mind and gives us a greater sense of infinity than if we
were to spend all our days with our eyes hypnotically glued to the giant
telescope at Mt. Palomar. What we see ultimately is that the placebo isn't
really necessary and that the mind can carry out its difficult and wondrous
missions unprompted by little pills. The placebo is only a tangible object made
essential in an age that feels uncomfortable with intangibles, an age that
prefers to think that every inner effect must have an outer cause. Since it has
size and shape and can be hand-held, the placebo satisfies the contemporary
craving for visible mechanisms and visible answers. The placebo, then, is an
emissary between the will to live and the body.
(Norman Cousins - who cured himself
of the medically incurable ankylosing spondylitis)
In an earlier study entitled Intention: Reality’s Hidden Force the observation had
been made:
[Perhaps there is
something behind what traditional shamans and healers have alleged: that our
brain-minds are very powerful, and that through intentionally projecting
internal images, we can instruct our bodies in the making of image-patterns for
more holistic bodies for ourselves. In this regard, there is also a great deal
of ongoing scientific interest in the bio-medical placebo effect, and
the results of our research on this topic will be shared in a future essay.]
…and
it is our hope that our findings will assist others in formulating their own
understanding of Nature’s Life-Management System.
Akin
to the processes of recombinant DNA whereby each of us has his or her own
unique molecular structure, so we each also have our discrete, interior
interpretation of reality and of our life and its meaning. This personal
interpretation expands as we mine our own experiences and those reported by
others. Yet no matter how ‘faith-based’ or ‘science-based’ others’ reports are,
those reports remain the property of the others, and cannot be taken at the
same level as one’s own experiences. Further, one’s interpretations of last
year may vary from those of today, for hopefully we learn as we age, and what
was anomalous before may – with additional experiences added to one’s book of
life – kaleidoscope into patterns allowing the emergence of deeper
understandings of some of the mysteries of life and life’s embodiment processes
and its ultimate passing.
Personally,
it has not been enough for us two to only know “what is …”, we want to
know “why?”… in other words, what is the process?? Concerning health issues, we
ourselves have tried to adhere to the principles expressed in “A Personal Mission Statement” by Ivan Illich
(Austrian
philosopher, Roman Catholic priest, and maverick social critic) who argued that medicalization had frequently caused more harm
than good and rendered many people in effect lifelong patients. As Illich
states, “we need the
courageous virtue to face certain truths:
·
we will never eliminate pain;
·
we will not cure all disorders; and
·
we will certainly die.
“therefore, as sensible
creatures, we must face the fact that the pursuit of health may be a sickening
disorder. There are no scientific, technological solutions. There is the daily
task of accepting the fragility and contingency of the human situation.”
In
our ongoing internal conversations, the concept of meaning arises again
and again, and we feel that it is our perennial responsibility to enhance the
‘tool-kit’ of cognitive concepts whereby we are able to mine our experiences
for value. Three such tools are the Powers of Tested Belief, of Intention, and
of WORDS being highly suggestive
and evocative.
The
concept of the evocable Internal Healer as revealed by the Placebo studies is
certainly not new to anyone who has studied the processes of shamans and curanderos
or to those called to serve as healers in long-established Amerindian, East
Indian and Chinese cultures. Some recent findings in our own culture have long
been common-sense elsewhere. For instance, it was a surprise to western
travelers to India that some yogis were seemingly not affected when given
massive doses of LSD and mescaline; the yogis explained that they were
accustomed to the mentally, self-induced effects of higher potencies,
endogenous neurochemicals required to put themselves into highly altered states
of consciousness so that they could move, cure and heal others. Seemingly,
these magi carried – in their own brains – their own internal
pharmacopoeia, from which they could compound the substances required to
transform themselves and thereby – through their presence, words, and rituals –
have curative effects on the afflicted.
Granted,
the prospect of individuals in our culture being conditioned to gradually
self-empower themselves through diminishing dependency on practitioners of the bio-medicine
model of slash, burn and poison protocols (scalpel, radiation and
pharmaceuticals) is a refreshing step in the right direction. A step. Yet
ultimately one has to ask himself what is his life really about… to whence does
one take his healthy body, and how does one use his short lifetime to make a
difference. And further, what is the qualitative difference in a person’s life before
and after his affliction, that makes his experience of illness and
restoration really worthwhile (to anyone other than members of the
‘health-care’ industry)? Why – even
after a most serious life-threatening experience – do some continue as before, responding to sanctioning cues from their social environment rather than
their internal guide; and – rather than becoming a healing placebo to others –
the recovered one persists in being a nocebo in others’ lives??
It is estimated that
60/70% of today's psychological problems are directly because of existential
reasons, wherein a person loses a sense of his unique, personal mission in
life, or becomes deeply confused as to how to organize his life so as to
acknowledge his life goal and move towards it. Unless a person can ‘reset’
himself mentally, he can become very apathetic and worn-down, and in the
process his immune system becomes adversely affected, firstly in acute physical
dysfunction, then at the chronic level. In applying his philosophy of Logotherapy,
the psychotherapist Viktor Frankl
found that many people had 'lost' their personal sense of meaning –
their unique, personal goals in life, and they expressed dysfunction firstly at
the psychological level, and if that can’t be turned around, then they often devolve
to states of chronic somatic illness. He therefore sought to re-establish in
his patients’ lives the will for meaning of their existence at
the deepest, or spiritual, level.
One aspect of the Frankl approach entailed a refocusing of the patient's
attention so as to restore confidence in his own self-curative powers, rather
than developing dependency on the alleged curative powers of others.
In
their work and writings, the famous therapist Carl Jung
and the motivational guru Abraham Maslow both used the term anhedonia
to classify the process whereby people experience this profound sense of valuelessness, when their lives seem without purpose or joy
or meaning either to themselves or to others. Jung explained that one’s shadow – a deep
aspect of the psyche – if repressed, can turn against oneself and create
nihilism and negativity. In like vein, Maslow said that evil is one’s
own ignorance when neglecting one’s own potential; that by not realizing one’s
potential but rather wasting it, the potential decays and brings disease; that
what one does not nurture and grow within might turn against one. Both Jung
and Maslow claimed that the process of self-empowerment began with
self-discovery and then attainment of self-realization (Jung) or
self-actualization (Maslow).
People
involved in motivational and industrial work would be familiar with the first
five levels of Maslow’s Heirarchy of Human Needs, and the main
hurdle for many people occurs in their being able to move beyond level two.
[Note:
neuroscientists feel that anhedonia appears to coincide with breakdown in a key
process in the Internal Healer’s reward system, involving the neurotransmitter
dopamine]
While
we can be grateful for the advances of the bioscience institutions, there is
yet something missing in the lives of many survivors. The natural healer of
older cultures seemingly picked up on messages of deeper, richer meaning from his
magical world. He had come to see life’s natural progressions and rhythms, and
the Great Spirit personally informed him as to Its need for his human
role in the co-designer/ co-creator/ co-healer pageant. Wherever such a natural
healer gazes, the Great Artist of his cosmology whispers “intelligence”
to him, and he knows that all of nature is alive and directing his attention to
the Miracle and Mystery of Life. The forests and the plains and the creatures
therein all honour his presence, and he is in harmony with the changing
seasons: the sun’s healing rays and the beauty of moon, stars and aurora
borealis all bespeak their need for his involvement.
The shaman/ yogi healer is different, and
those under his care also become different through having being touched by his
mind and presence, and from his assurances that they too are needed in the
Great Spirit’s plan. And so, when the patients of these natural healers
are restored, they in turn are also changed. Instead of becoming ever more
hubristic members of an exploitive, materialist society through reliance on the
wielders of scalpel and poison for their restoration – they realize that –
through the agency of their natural healer – they have personally gained
insights of self-empowerment as a result of their illness; having been guided by
their healer in the encounter in the Great Mystery, they have discovered
themselves worthy of going forward in health, duty-bound to help others.
Many of those reporting above on placebos refer
to the self-healing effect arising from a ‘meaning response’, wherein
practitioners of any modality through their rituals of intention and
interaction convey to their patients that their lives are meaningful, and that
they are valuable and worthy of restoration. In our day-to-day involvement in
our social worlds, our interactions with those personally important to us also
fulfill this function through conveyance to us of their need for us in
their own lives; and where there is a sense of our being needed - we naturally
strive to rise to others’ need by endeavouring to be present in response. Where
one senses that one is needed and one’s existence is meaningful to others, one
feels duty-bound ‘to show up’.
Just
as one’s own constitution contains mechanisms such as the Internal Healer to
sustain and enrich one’s life, the constitution of a society also contains
mechanisms for the harmonization of relationships amongst its members; the
protocols of honouring others rather than signaling meanness and estrangement;
of practicing dialogue rather than aggression and violence; of appreciating and
respecting diversity rather than insistence on sameness – in these ways we can
all honour our uniqueness, whilst fulfilling our roles as placebo healers in
the greater social pageant.
Once we realize our innate faculty of participating
in the harmonization of our own personal health, the challenge moves to the
stage of our society and the healing of dis-ease in the lives of our brothers
and sisters – and then a meta-vision comes to our wondering minds as to
the real intention behind Nature’s Life-Management System.
(PiPS)* - The Harvard based Program in Placebo Studies (PiPS) group includes
anthropologists, sociologists and psychologists who conduct research into
placebo effects and the therapeutic relationship; the team investigates how the
power of imagination, ritual, symbols, meaning, empathy, hope, compassion and
trust – what can collectively be called the “moral imagination” – are
translated into clinical outcomes and better health. There is a fascinating documentary entitled [RIGHT CLIK FOR NEW TAB] Placebo: Breaking The Code about the science and psychology of placebos, centered on a gathering
of the Harvard Placebo Study Group at a remote cottage in Ireland. Featuring
Nicholas Humphrey, Anne Harrington, Dan Moerman, Howard Fields, and Fabrizio
Benedetti.
(1) The Association for Research and Enlightenment (A.R.E.) is in
Virginia Beach, and is the fruit of the vision of Edgar Cayce, a unique psychic
who had became famous in the period 1935-50 for his seeming ability, under
light hypnotic trance, to diagnose and prescribe for requesting patients at
remote distance. The A.R.E. public libraries contain some 60,000 books by
premier philosophers, consciousness researchers, medical practitioners, etc,
and also cover esoteric aspects of world belief systems; there are also many
very rare collections protected in temp-humidity controlled rooms, access to
which is closely monitored. A.R.E. also functions as a mecca for people from
around the world seeking to learn more of the deeper aspects of life – usually
because of some personal transformative experience – thus there were many
opportunities to compare findings with others.
(2) from UCLA study - Brain Imaging Study Reveals
Placebo's Effect http://www.placebo.ucla.edu/news/PDF/sciam020102.pdf
(3) 22-12-2010
interview with Steve Silberman “Meet the Ethical Placebo: A Story that Heals”…
more at http://blogs.plos.org/neurotribes/2010/12/22/meet-the-ethical-placebo-a-story-that-heals/
(4) For further quotes from The Emperor's New Drugs: Exploding the
Antidepressant Myth by Irving Kirsch, see http://www.goodreads.com/author/quotes/432088.Irving_Kirsch
(5) From Placebo studies and ritual theory: A comparative analysis of Navajo,
acupuncture and biomedical healing - Links to additional Kapchuck publications can be accessed via http://tedkaptchuk.com/selected-publications
(6) From Ted J. Kaptchuk et al ‘‘Maybe I Made
Up the Whole Thing’’: Placebos and Patients’ Experiences in a Randomized
Controlled Trial”. Full paper (pdf) at http://g.virbcdn.com/_f/files/91/FileItem-110498-MaybeImadethewholethingup.pdf
(7) From
Ted J.
Kaptchuk et
al “Placebos without Deception: A
Randomized Controlled Trial in Irritable Bowel Syndrome” at [RIGHT CLIK FOR NEW
TAB] http://www.plosone.org/article/info:doi/10.1371/journal.pone.0015591
(8) From Fabrizio Benedetti et al “Neurobiological Mechanisms of the Placebo
Effect” at [RIGHT CLIK FOR NEW TAB] http://www.jneurosci.org/content/25/45/10390.full
(9) From
article “The Nocebo Effect” at http://www.guardian.co.uk/science/2011/nov/13/nocebo-pain-wellcome-trust-prize?newsfeed=true
(10) From “Deconstructing
the Placebo Effect and Finding the Meaning Response” by Daniel E. Moerman, PhD,
and Wayne B. Jonas, MD, at
http://www-personal.umd.umich.edu/~dmoerman/aim_plac.pdf
(11) These clips were drawn from Nicholas Humphrey’s full
paper “Great Expectations: The Evolutionary Psychology of Faith Healing and
The Placebo Effect” at http://www.humphrey.org.uk/papers/2002GreatExpectations.pdf;
An EDGE conversation with Humphrey can also be
found here, and his personal web archives are here
(12) These clips were drawn from Setting the Stage for Pain - Allegorical Tales from Neuroscience by Professor Fields.
See also his Lecture at Berkeley
"Origins of Pleasure and Pain" mp3
(43 min) and QA
(4 min); and his participation in the Harvard Placebo Study
Group’s [RIGHT
CLIK FOR NEW TAB] Placebo: Breaking The Code.
(13) From “The Triumph Of New-Age Medicine” by
David H. Freedman - Atlantic Magazine July-Aug 2011, at http://www.theatlantic.com/magazine/archive/2011/07/the-triumph-of-new-age-medicine/8554/1?single_page=true
Posted January 18th, 2012
Keith and Marnie
Elliott’s “REMEDY” Site
Home
|
Our Stories |
The Sublime |
Our World and Times |
Book Reviews
|
Marnie's Images |
The Journal |
Gleanings |
From The Writings Of. . . |
Allegories |